Overview
Children and young people are different from adults. They are continually developing physically, emotionally and psychologically. Due to the physiology and biomechanics of growth, young people show a unique set of age related symptoms. Whilst many conditions seen in childhood are self-limiting; some more serious pathology can occur. As a specialist Musculoskeletal Physiotherapy team we hope that you find the information on our website helpful, but if the pain your child is experiencing does not improve please seek further medical advice and if its deemed appropriate your GP can refer your child to our physiotherapy service.





Knee Pain
If your child has experienced trauma related onset of knee pain i.e. knee pain that started after a trip, slip, fall or contact with another person or object, and there is immediate swelling and bruising that occurs within 20 minutes of the injury, then we would recommend you seek immediate advice from a medical professional.
If your child is experiencing knee pain that was brought on by trauma, but without immediate swelling and bruising, but the pain has persisted for more than a few weeks without showing signs of improving, we would also recommend seeking expert medical advice. In most cases we would expect such injuries in a fit and healthy child to settle within a few weeks with appropriate rest, ice and if required elevation.
If your child starts experiencing knee pain without a known mechanism of injury and there is swelling, redness or increased temperature to the area, please seek medical advice.
If your child starts experiencing knee pain without a known mechanism of injury and it does not get better within a few weeks, again seek medical advice.
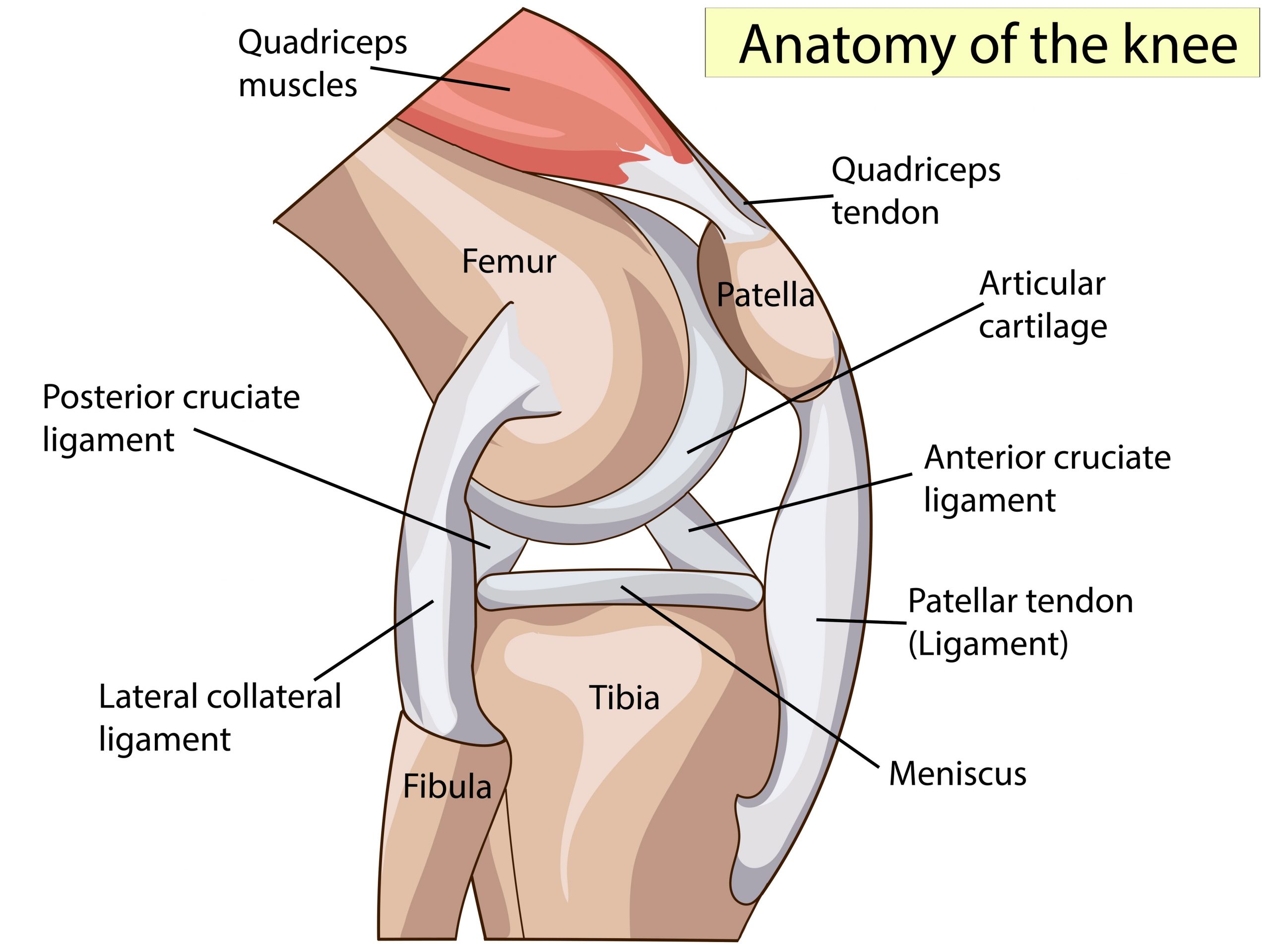
Anterior Knee Pain
Anterior knee pain is a common term used to describe pain at the front centre of the knee. It should not be confused with pain located in the upper shin bone (just below the knee cap) because this is a different condition called Osgood Schlatter’s disease, and there is often an associated bony lump.
Anterior Knee pain can also sometimes be referred to as Chondromalacia Patellae or Patella Femoral pain syndrome. It can occur in both children and adults, but is common in adolescents, especially around periods of rapid growth or with increased sports participation. It is more common in girls than boys. It often occurs in both knees, but can affect just one.
It can often be difficult to give one particular explanation for Anterior Knee pain. It is not usually caused by a defect in the knee, but may be due to;
- an imbalance in muscles around the knee
- weakness in muscles around the knee
- tightness in the quadriceps and hamstring muscles
- altered bio-mechanics (poor alignment of hips, knees, ankles & feet)
- an overuse injury caused by high intensity training
- poor footwear
- poor running technique
The pain will usually come on gradually and be described as a dull ache. It is often made worse by certain activities such as running, jumping, walking down stairs or a steep hill.
In most cases Anterior Knee pain will settle with rest, ice or simple analgesia. It is also important to ensure good supportive footwear is worn especially school and sports shoes. However, if the pain persists beyond a few weeks then you should contact your GP or Physiotherapist and they can assess the area. They may give some exercises to help strengthen and/or stretch specific muscles.
Exercises that may help:
- Quads Stretch
- Hip flexor stretches
- Squats
- SLR
- Lunges
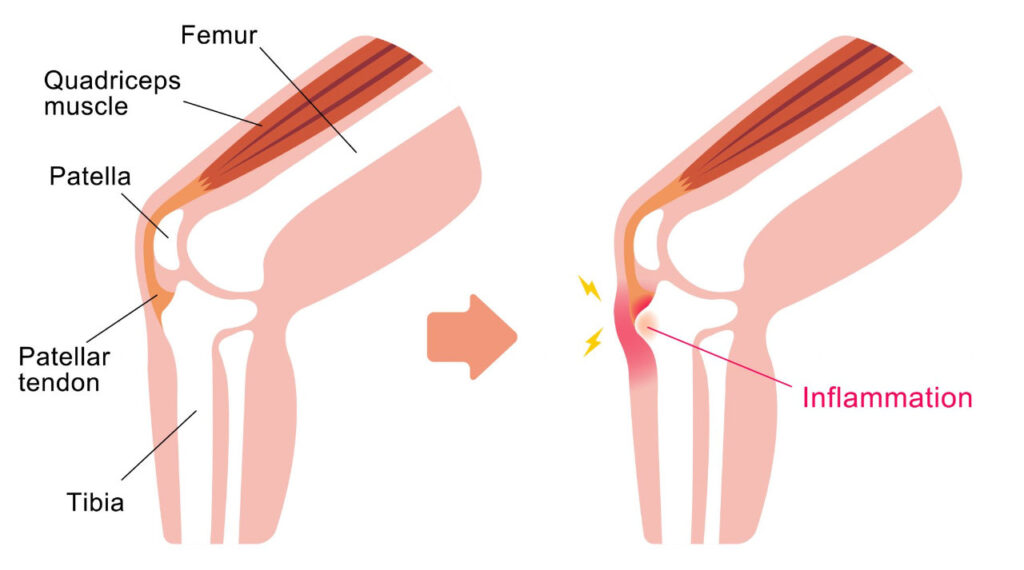
Osgood Schlatter’s Disease (OSD)
OSD is a common cause of knee pain in children and adolescents, especially those that are very physically active and do a lot of running, jumping or kicking sports.
OSD is caused by swelling and irritation of the growth plate at the top of the shin bone. Growth plates occur at the end of bones and as the name indicates, it is where the bone grows from. When the young person reaches skeletal maturity (stops growing) the growth plate fuses and no more growth occurs. This process is usually complete by the age of 25 years, but can vary significantly and usually occurs earlier in girls than boys. The pain is caused by a sudden growth spurt in a physically active child. During a period of rapid growth, the bones, muscles and tendons can grow at different rates. In OSD, the tendon that connects the shin bone to the kneecap pulls on the growth plate at the top of the shin bone (just below the kneecap). It is this pulling that causes the pain and irritation associated with OSD. In some cases, the repeated pulling on the soft growth plate bone causes it to bulge and can be felt as a hard lump under the skin in the area.
OSD typically causes pain and swelling below the kneecap. The pain usually gets worse with running, jumping, going up stairs, and walking up hills. Severe pain may lead to limping. OSD can happen in one or both knees. OSD rarely causes any long-term knee problems that continue into adulthood, because once the child stops growing the muscles ‘catch up’ with the bone growth and the growth plate hardens, both of which result in the cessation of the traction and irritation.
Young people with OSD can carry on playing sport and being active if they can tolerate the pain associated with it. If, however the pain is causing a limp then it is sensible to rest until the pain settles. This will often take a couple of days, they can then resume sport as pain allows.
OSD will usually be eased by;
- Rest
- Ice or cold pack on knee every few hours for 15 min at a time. Put a thin towel between the ice and knee to protect the skin from an ice burn
- Stretches of the quadriceps especially before and after sport and more regularly during growth spurts
- Non steroidal anti – inflammatory gels may also be helpful.
Useful Links
- For further information on posture mistakes and fixes click here.
- Click here to find out facts about what food you are eating
- Find out if your child is at a healthy weight
- Guidance on the types and amount of physical activity children should be completing to stay healthy.
- Take a look at some fun exercise activities you can do at home you’re your children