Overview
Children and young people are different from adults. They are continually developing physically, emotionally and psychologically. Due to the physiology and biomechanics of growth, young people show a unique set of age related symptoms. Whilst many conditions seen in childhood are self-limiting; some more serious pathology can occur. As a specialist Musculoskeletal Physiotherapy team we hope that you find the information on our website helpful, but if the pain your child is experiencing does not improve please seek further medical advice and if its deemed appropriate your GP can refer your child to our physiotherapy service.





Foot & Ankle Pain
If your child is experiencing foot and/or ankle pain, and you are not sure why, have a good look at their shoes. Good supportive shoes and trainers can make a big difference to aches and pains in hips, knees, ankles and feet. This is especially true if your child does not have ‘neutral’ biomechanics. By this we mean optimal alignment of their legs and feet. Sometimes this is quite obvious and sometimes it is more subtle. Looking at the soles and wear distribution of your child’s shoes can give some indication.
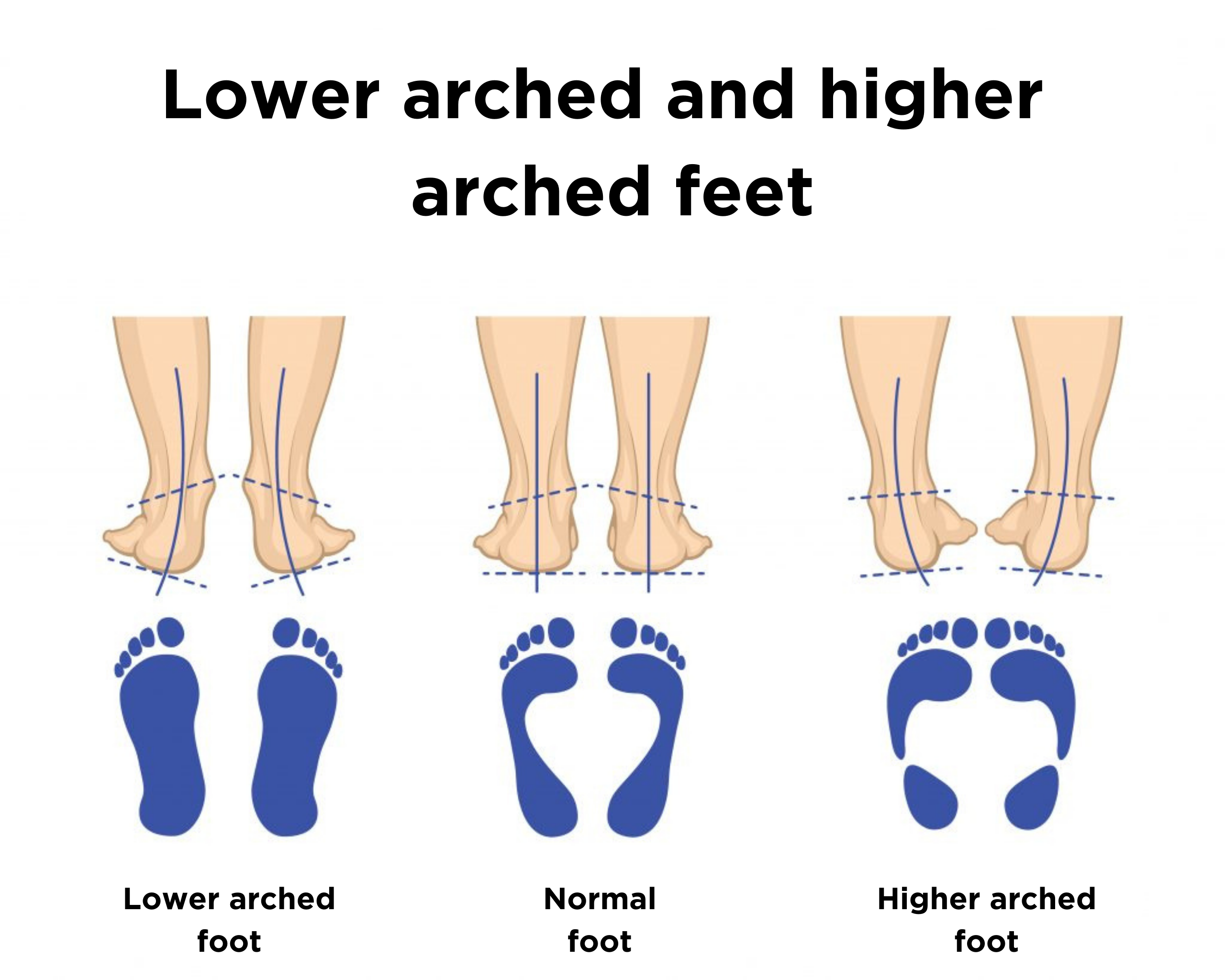
Issues with the Arch
The arch, or instep, is the middle part of the foot that’s usually raised off the ground when you stand, while the rest of the foot remains flat on the ground. In young children, this arch isn’t always visible because of the baby fat and soft tissue in their feet. It usually develops and appears by the age of 7-9 years old. However, some people never really develop this arch. Sometimes, this is because they inherited lower arches (flat feet) from their parents.
People with flat feet, low arches, or overly flexible arches tend to roll inward, this can twist the foot, leg and knee causing poor alignment and sometimes pain. Flat feet also mean the big toe and one next to it take on more of the effort during the push off part of your step and this can also sometimes lead to pain and the development of bunions in later life.
Many people simply inherit flat feet from their parents, but it can also be aggravated by connective tissue in the foot becoming stretched and inflamed – possibly as a result of overuse, unsupportive footwear, an injury, increasing age, obesity or rheumatoid arthritis. Occasionally, flat feet can be the result of the feet bones not forming properly in the womb or loose connective tissue throughout the body.
Flat feet only need to be treated if you have an associated problem, such as pain or you are concerned your child’s feet are extremely flat (the whole of the foot is in contact with the floor). Non-surgical treatments, such as the recommendation of good supportive shoes and orthotics (in soles) are often recommended in the first instance and in most cases is all that is needed. Surgery is rarely required and only in the most severe of cases.
High arched feet are the opposite to flat feet, and is less common. It can cause the foot to roll outwards so more of the load is going through the little toe and down that outer edge of the foot. This can lead to foot, ankle, knee, hip and back pain.
Often the higher arched foot is associated with tight Achilles tendons and calf muscles, so calf stretches can help. It is important to wear good supportive shoes that have an arch support in them, and in more severe cases orthotics (insoles) to support the arch of the foot may be helpful.
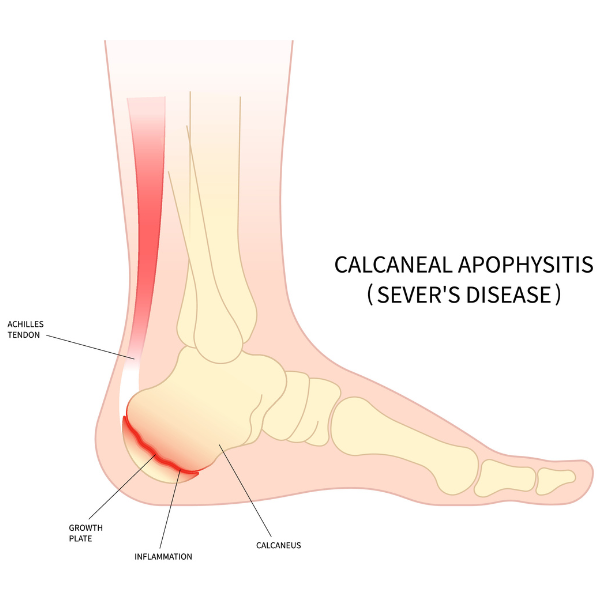
Calcaneal Apophysitis (Sever’s Disease)
Sever’s disease is a painful condition of the heel that occurs in growing children. It happens when the tendon that attaches to the back of the heel (the Achilles tendon) pulls on the growth plate (the apophysis) of the bone of the heel (the calcaneus). The repeated stress on the growth plate causes pain and inflammation at that site. It typically affects children between the ages of 8 and 14 years old.
It is the most common cause of heel pain in children, and can occur in one or both feet.
While painful, Sever’s disease is not a serious condition. It will not cause long term damage or arthritis and often resolves once the growth plates close.
Sever’s disease is more common during periods of rapid growth when the bones grow faster than the tendons. This increases the pull of the tendon on the heel bone. Pre-existing tight calf muscles increase the likelihood of the condition, as does high volumes of impact sports. The heel’s growth plate is sensitive to repeated running and pounding on hard surfaces, resulting in muscle strain and inflamed tissue. Other potential causes of calcaneal apophysitis include obesity and biomechanical problems such as flat foot or a high-arched foot.
Symptoms of calcaneal apophysitis is pain in the back or bottom of the heel. The pain may come and go over a prolonged period of time and often be related to increased activity. The pain may cause children to limp, walk on their toes, difficulty running, jumping or participating in usual physical activities.
- Rest: Limit physical activities, especially running and jumping, while having pain. Take rest breaks between activities. If your child is able to keep playing sport it is ok to do so.
- Ice: Ice the heel for 15 to 20 minutes when having pain or after activities. Do not place ice directly on skin. Put a towel or other cloth between the ice and the skin.
- Footwear: Always wear a well-cushioned pair of supportive shoes. Do not walk in bare feet. In some cases, special gel inserts for the shoe called heel cups may help.
- Stretches: Stretching the calf muscles can help loosen tight Achilles tendons and help decrease the pull of the tendons on the growth plates.
Hold each stretch for 30 seconds. Repeat 10 times. Try and do this stretching 3x a day – when you get up in the morning, when you get home from school and before bedtime.
Recovery from Sever’s disease varies from patient to patient. In most cases, Sever’s disease goes away on its own with rest, treatment, and time. Symptoms may worsen if your child tries to play through the pain but this should not cause any long-term problems with the foot or ankle. The pain may come and go over a period of years (typically between the ages of 8-14 years). However, the pain should not continue beyond fusing of the growth plate. Your child should continue with calf stretches regularly to try to help prevent re-occurrences.
Useful Links
- For further information on posture mistakes and fixes click here.
- Click here to find out facts about what food you are eating
- Find out if your child is at a healthy weight
- Guidance on the types and amount of physical activity children should be completing to stay healthy.
- Take a look at some fun exercise activities you can do at home you’re your children